RWE Mastery: From Real-World Data Capture to Evidence-Based Decision Making

DATE
June 18, 2024
AUTHOR
Catherine | Associate Director Marketing
The following is a transcript of a joint webinar with Hendrik Stork (IQVIA) which was hosted by Climedo on March 13, 2024.*
Introduction
Welcome, everyone. Today, we will explore the realm of real-world data (RWD) and evidence (RWE), breaking it down into four main buckets:
1. What is Real-World Data?
2. Why Real-World Data and Evidence?
3. How to access Real-World Data
4. Driving Evidence-Based Decision Making
We’ll focus specifically on RWD within the context of the healthcare system, steering clear of other industries where RWD may hold different significance.
1. What is Real-World Data?
Real-world data in health economics can originate from two types of sources:
- Secondary data collected for purposes other than specific research objectives
- Primary data collected for specific purposes not available from existing resources
This data can encompass patients’ health status and the delivery of healthcare treatment, sourced from various channels or combined. The goal is always RWE generation, achieved through interpretation and analysis via specific study design methods. This provides outcomes and evidence on the usage, for instance, of a certain medical product’s benefit and risk profile.
Although clinical evidence is also part of the broader evidence generation spectrum, today we will focus primarily on RWE. Evidence can also come from clinical trials, including randomized trials, pragmatic RCTs and low interventional clinical trials, which are becoming more and more intertwined with RWE. More studies are being requested in the realm of low-interventional clinical trials. These fulfill the requirements of real-world observational studies to some extent, but are classified as low-interventional clinical trials due to randomization.
RWE comprises both prospective and retrospective data, with primary data collection and utilization of existing data sources leading to time and cost savings as well as reduced complexity. This aligns with the trend of focusing more on existing data sets and exploring possible ways to collect them. These sources can range from claims databases, consumer data and observational studies to electronic medical records, pharmacy data and social media data, reflecting the interconnectedness of the healthcare ecosystem.
Live audience poll: What is your RWE experience?
Results:
- 16% have no experience
- 54% have some experience
- 30% work with it regularly
2. Why Real-World Data and Evidence?
Let’s move on to the second chapter: Why real-world data and evidence? For those of you who have already worked with them, you most likely understand their value. It’s always a matter of perspective, but three major perspectives include:
- Healthcare providers
- Industry
- Regulatory bodies and payers

In Zurich, the number of departments required to collect patient-reported outcomes (PROs) depends on their size. They aim for a mandatory collection of relevant patient-centered quality parameters for further assessment and data warehousing. Subsequent requests for proposals followed for dat warehouse set-up, with insurance providers also participating in discussions. Switzerland’s implementation strategy and value-based approach to healthcare reimbursement appear advanced compared to Germany. Despite differences in speed, Germany learns a lot from Switzerland’s advancements in healthcare initiatives.
In all these examples, the involvement of the University of Basel and the Swiss health system was prominent. They collaborated extensively, adapting to changing requirements.
Lastly, I’d like to highlight the significance of registries. Registries come in various forms, such as those set up with medical societies or pharmaceutical companies. For instance, I collaborated on setting up a breast cancer registry with 15 hospitals in Germany, focused on collecting relevant data for research and treatment improvement. Other registries may focus on product-related observational studies, aiming to demonstrate additional benefits over competitors.
The character and scope of registries depend on various factors, including funding, involvement of industry sponsors and research questions. Regardless of their nature, registries offer valuable data for product development, market access and regulatory compliance. They help answer crucial questions about target markets, optimization of trials, market readiness and branding strategies. Utilizing RWE early in the product lifecycle is crucial, particularly during product launches, to ensure successful market penetration and adoption.
RWE usage tends to peak during product launches, emphasizing the importance of early consideration and integration of RWE into market access and commercialization strategies. RWE continues to drive return on investment throughout the development phase and beyond, influencing medical messaging and sales efforts aimed at persuading physicians to adopt products. Overall, RWE plays a vital role in driving success in the pharmaceutical and healthcare industries.
RWE will aid in several key areas, including:
- Developing an informed strategy
- Understanding patients’ unmet needs
- Defining subgroups for clinical development
- Accelerating and optimizing trial designs
- Securing data-driven feasibility and recruitment strategies
- Establishing endpoints
- Supporting label expansion
- Health Technology Assessment (HTA) submissions, pricing and reimbursement negotiations
- Demonstrating comparative advantages
- Informing clinical guidelines
- Maximizing asset value
- Accelerating timelines and saving costs.

Live audience poll: Where do you think RWE offers the highest potential? (multiple choice)
Results:
- 69% say post-approval value
- 56% say optimizing care pathways
- 49% say HTA / Market Access
- 42% say enhancing clinical development
- 36% say informed strategies
- 29% say label expansion
It’s interesting to see that post-approval value and optimizing care pathways were the top choices among the audience.
Moving on, I’d like to conclude this segment with some recent data, which can be found in an IQVIA whitepaper (Launch Excellence VIII Whitepaper; “Excellent launches are winning the evidence battle”). The paper highlights a significant decline of over 23% in successful launches since pre-COVID times, emphasizing the need for a turnaround strategy.
Three critical success factors have been identified:
- Real-World Evidence (RWE): Early generation of RWE has consistently led to more successful launches. Utilizing RWE pre-approval can significantly enhance the launch process.
- Sharing RWE and insights: Providing healthcare providers with relevant insights, such as additional medical benefits and safety profiles, can drive decision-making and engagement with treatments.
- Patient awareness: Patients need to be informed about the additional benefits of treatments, which can enhance their engagement and adherence.
These factors underscore the importance of leveraging RWE to optimize launch strategies and improve the success rates of pharmaceutical launches.
The timing of sharing study insights is currently far too late. Patients may only receive knowledge about the benefits and potential side effects of a medication 18 months after its launch, despite having been taking the medication for a significant period. This delay can lead to missed opportunities for earlier treatment changes that could have resulted in better outcomes. Therefore, it’s crucial to address this issue and ensure that study insights are disseminated in a timely manner to both patients and healthcare professionals (HCPs).
These insights form a critical triangle, where each factor influences the other. Patients can only be informed if HCPs have access to relevant information. Thus, finding new ways to engage with and exchange information with HCPs becomes essential, especially considering the decline in interactions post-COVID-19. Despite this decline, medical information remains highly sought after by physicians, underlining the importance of effectively delivering this information.
3. How to Access Real-World Data
This leads us to the third aspect of today’s session: accessing Real-World Data (RWD) in general. The choice of data source heavily depends on the indication and specific requirements.
In general, secondary data are analyzed based on existing, mostly analyzed data, making them readily available and usually not requiring ethical approvals. They offer simplicity in feasibility and operations, with less complexity and greater cost efficiency.
On the flip side, secondary data sources require thorough checks on data quality and completeness. They need validation processes and often lack crucial patient outcomes or other data points. In contrast, retrospective or prospective data can be tailor-made according to specific needs, ensuring the collection of relevant outcomes. The integration of patient-reported outcomes is feasible in such cases. Additionally, other variables from apps or smart fitness devices can be included if the technical infrastructure supports it.
You can also streamline data collection by working with different existing data sources within physician systems or clinics, such as electronic medical records. This approach makes data entry more efficient, as information only needs to be entered once into a single system that feeds into others. However, this method is more complex and requires elements like ethics submissions and patient consent forms, making it longer and more costly compared to database studies.
Setting up a registry can be approached in various ways, considering factors like technical infrastructure, partnership arrangements (e.g., with industry or medical societies), data protection measures, access rights and informed consent design. Additionally, establishing a neutral entity for data aggregation and analytics may be necessary for combining different datasets, although this adds complexity to the process. Despite these challenges, creating registries is feasible with careful planning and execution.
It’s great to hear about the experience with registries at IQVIA and within your department. Setting up a new registry may seem complex, but it’s indeed feasible and often more affordable than perceived.
Moving on to the next slide, let’s delve into more specific information, focusing on secondary data, retrospective chart abstraction and prospective data collection. These examples can vary depending on research objectives and needs.
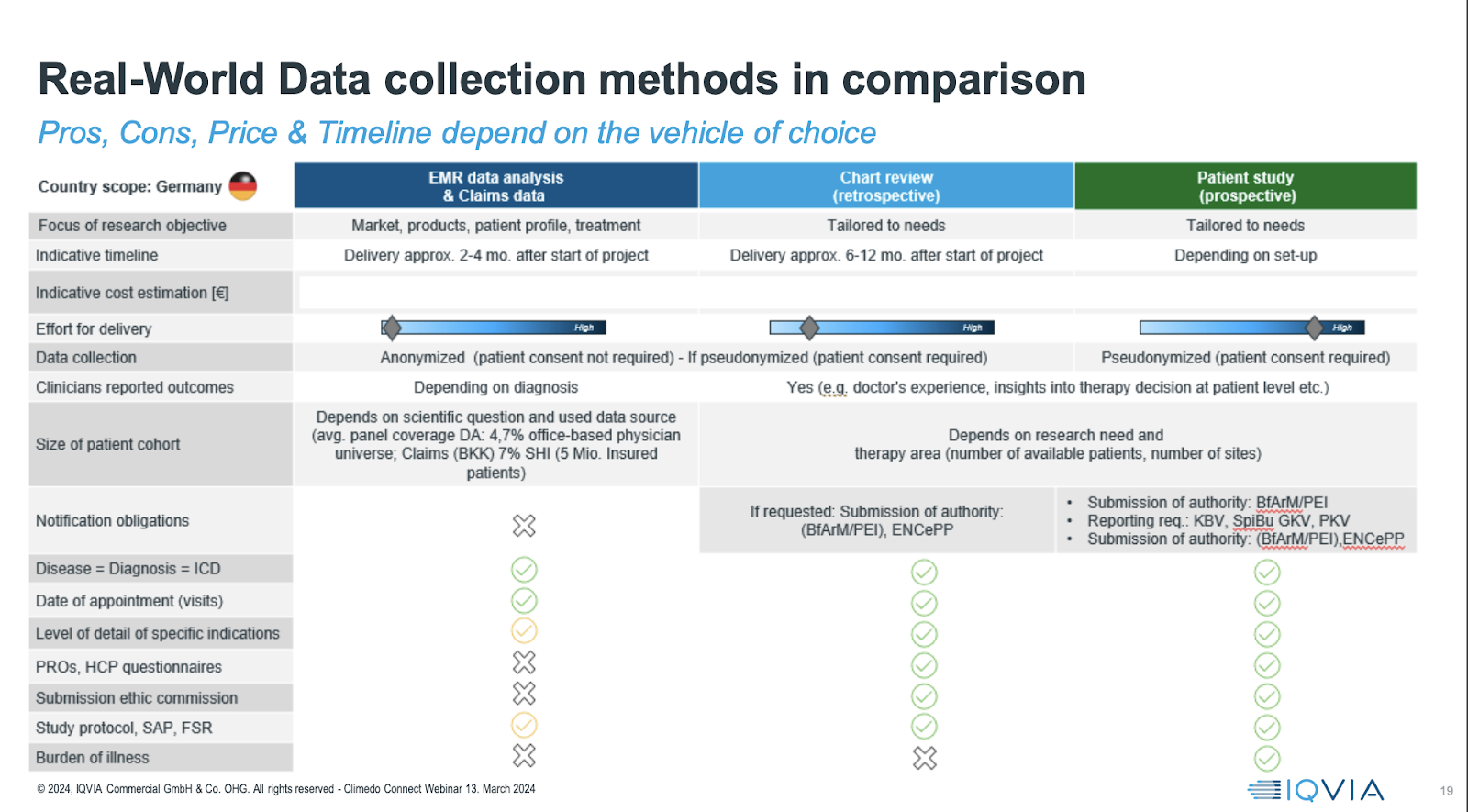
Secondary data sources, typically collected for market purposes, offer fast availability. Conversely, chart abstraction may take between 6 to 12 months or longer, depending on the number of sites involved and contracted. Prospective studies, on the other hand, can vary significantly in duration, ranging from one to five years or even longer, depending on setup, data collection needs and observational periods.
Certainly, it’s important to note that the numbers provided are for reference purposes only and not set in stone. The timeline and cost of setting up studies can vary significantly depending on factors such as the indication area and whether it involves rare diseases, which can add complexity.
In the prospective context, the timeline and cost heavily depend on the number of sites and patients involved. Multi-country studies are feasible, but the scope can influence the resources required. For instance, a single-country German study with approximately 20 to 25 sites and 300 to 500 patients might cost between 1 and 2 million, as a reference.
Additionally, it’s crucial to consider ethical requirements, especially regarding consent and the size of patient cohorts, which vary based on research needs and study design.
Considering feasibility is crucial to ensuring that the study objectives are achievable within a reasonable timeframe and resources. Determining what is reasonable to expect with a specific number of sites and patients within a defined recruitment period is essential for planning prospective data collection.
While prospective data collection requires regulatory submissions, it offers several advantages. It provides detailed information on disease diagnosis, ICD coding, appointments and a granular level of detail for specific indications. Moreover, prospective studies allow for the inclusion of clinical outcome assessments and patient-reported outcomes, enabling the development of a comprehensive study protocol and analysis plan.
However, it’s essential to balance the advantages with the investment of time and resources, considering the specific needs and objectives of the study. This evaluation helps determine the most suitable approach for achieving the desired outcomes.
Observational studies offer flexibility in tailoring the study design according to specific data needs and outcomes. This flexibility allows for cost-efficient approaches, where certain services can be managed internally, leveraging existing technology and resources.
For instance, if you already have data collection technology in place, you can handle data collection internally. Similarly, if you have sales or medical representatives who can support site monitoring and assistance, you can utilize them for those tasks. Parts of the analysis and method interpretation can also be conducted internally, depending on the expertise available within the organization.
Setting up an observational study involves several key steps, including protocol development, regulatory compliance, data collection, analysis and interpretation. While regulatory requirements may seem challenging, they are manageable with the right approach and support from partners.
Overall, observational studies can be structured in a way that aligns with available resources and requirements, offering flexibility in selecting appropriate packages and partners to achieve study objectives efficiently.
We are witnessing a shift in the way data is collected and utilized, with a growing emphasis on leveraging existing data sources and technologies. Here are some key trends we are observing:
- High Volume Site-Based Studies: While traditional site-based studies are still prevalent, there is a recognition of their time and cost intensity. However, they still play a role, particularly in innovative study designs and data-driven feasibility assessments.
- Data-Driven Feasibility and Study Designs: There is a move towards using data-driven approaches to inform study design and feasibility assessments. This helps in optimizing resources and improving study quality.
- Patient Engagement via Software Systems: Innovative methods for engaging patients through software systems are emerging. This not only enhances patient participation but also leads to higher quality data.
- EHR to EDC Integration: Efforts are being made to integrate electronic health records (EHR) with electronic data capture (EDC) systems. This integration streamlines data collection processes by identifying existing data sources and collecting missing data points.
- Remote Monitoring: On-site monitoring is gradually being replaced by remote monitoring or verification, reducing the need for physical site visits and minimizing disruptions.
- Increased Demand for Real-World Evidence: With regulatory bodies, payers and market access stakeholders increasingly recognizing the value of real-world evidence, there is a growing demand for such data in decision-making processes.
Overall, these trends indicate a shift towards more efficient and data-driven approaches in clinical research, leveraging existing data sources and technologies to enhance study quality and streamline processes.
Live audience poll: What is your experience in accessing and working with different data sources?
Results:
- 53% have worked with secondary and prospective data
- 27% have worked only with secondary data
- 16% have worked only with prospective dat
- 4% haven’t worked with either type of data.
It’s interesting to see that the majority of respondents have experience working with both secondary data and prospective data. This distribution of experiences suggests a well-rounded understanding of real-world evidence generation methods among the audience, with a significant portion having hands-on experience with both types of data sources.
4. Driving Evidence-Based Decision Making
Moving on to our final chapter: Once the groundwork has been laid for evidence-based decision-making, data collection alone is not enough without a plan. We can call it an integrated evidence strategy or label it differently, but essentially, it involves bringing together all the stakeholders’ needs, evidence requirements and available resources in relation to your product lifecycle and stages.
You need to have cross-functional team alignment to ensure that everyone’s needs are aligned, eliminating redundancies and increasing efficiencies to mitigate operational pitfalls. Only when there is consensus among the team across units can a strategy be implemented effectively, along with the necessary technology to maximize the real-world data and evidence generated.

It all starts with the strategy on the left. After that, you need to engage with the data sources. It’s encouraging to see that most people in the audience today have already worked with both secondary data sources, which need to be on the radar. Understanding what is already available and what additional data is needed is essential.
This is not just theoretical; it needs to be done with technology in place that not only collects but also processes and analyzes the data in a way that meets the needs of the stakeholders involved. This may require different dashboards for different departments, such as one for the sales department and another for the development department.
But it will help everyone to be on the same level with the same data collected. Beyond just collecting the data, it’s crucial to analyze it to derive evidence, which will automatically lead to medical messaging and impact. This can then be translated into a commercialization strategy that should be executed, measured and impact-evidence programs.
Now, diving a bit more into detail about the different capabilities that might be useful to fulfill those buckets: Of course, strategy was mentioned as well as everything related to drug development. Having a healthy pipeline nowadays is more important than ever. Looking towards the future, it’s not only about drug development but also considering multi-phase approaches for patient and provider engagement in product development.

Data landscaping has been mentioned multiple times; you need to know what data is available to avoid surprises and to ensure that you can access data quickly and securely. Proper advisory for regulatory, payer and pricing in your focus area is also definitely necessary to ensure that the right knowledge is in place.
I will stress this a little more on the next slide with regard to the technical implementation side of things. There are a lot of advanced technology options out there already: Artificial intelligence, machine learning, to name a few. You need to figure out what is needed for you to help get the value out of the data. Not everything is necessary, but some of it might be relevant and helpful.
On the right side of the slide, the publication planning and medical writing are not too much in focus, but I think we automatically nurture these with the analyzed evidence generated on the high-quality data collection. It will also help facilitate patient target evidence and communication and open up new doors to innovative contracting. This is currently done by insurances inviting hospitals, demonstrating their quality and getting reimbursed for it. Also not to forget the patient support programs.
And I like the very last one, medical KPIs. They are relevant, but I think most of you in the audience are already measuring them.
Emphasizing the technological aspect further, let’s delve into a brainstorm slide. Drawing from my experience, it’s crucial to establish both an idea and a strategy for accessing data effectively.

One avenue for this is health platforms. While IQVIA is readily available to offer support, it’s important to acknowledge that we’re not the sole solution. Various other platforms provide high-quality data, clinical outcome systems and electronic data capture systems integrated into broader healthcare ecosystems. These alternatives could enhance data collection and analytics capabilities.
Moreover, it’s essential to explore emerging platforms for dynamic analytics and scalable tools. These tools facilitate rapid analysis through technologies like machine learning or HTA accelerator programs. Unlike traditional methods that take weeks or months, these platforms deliver outcomes swiftly and efficiently, enriching trial designs and meeting evidence requirements.
For instance, natural language processing streamlines data analysis, while GDPR-compliant providers enable seamless integration of sensitive data sets, maximizing analysis value without constraints. While trust in these solutions may vary, initiating communication with such providers is advisable.
Now, let’s illustrate how this technology translates into everyday scenarios, based on an example from the Climedo platform. On the left, imagine a screen displaying health-related outcomes to a physician, with alerts triggered for abnormal thresholds. This enables proactive patient interaction and benchmarking against larger groups for collaborative learning and treatment optimization.
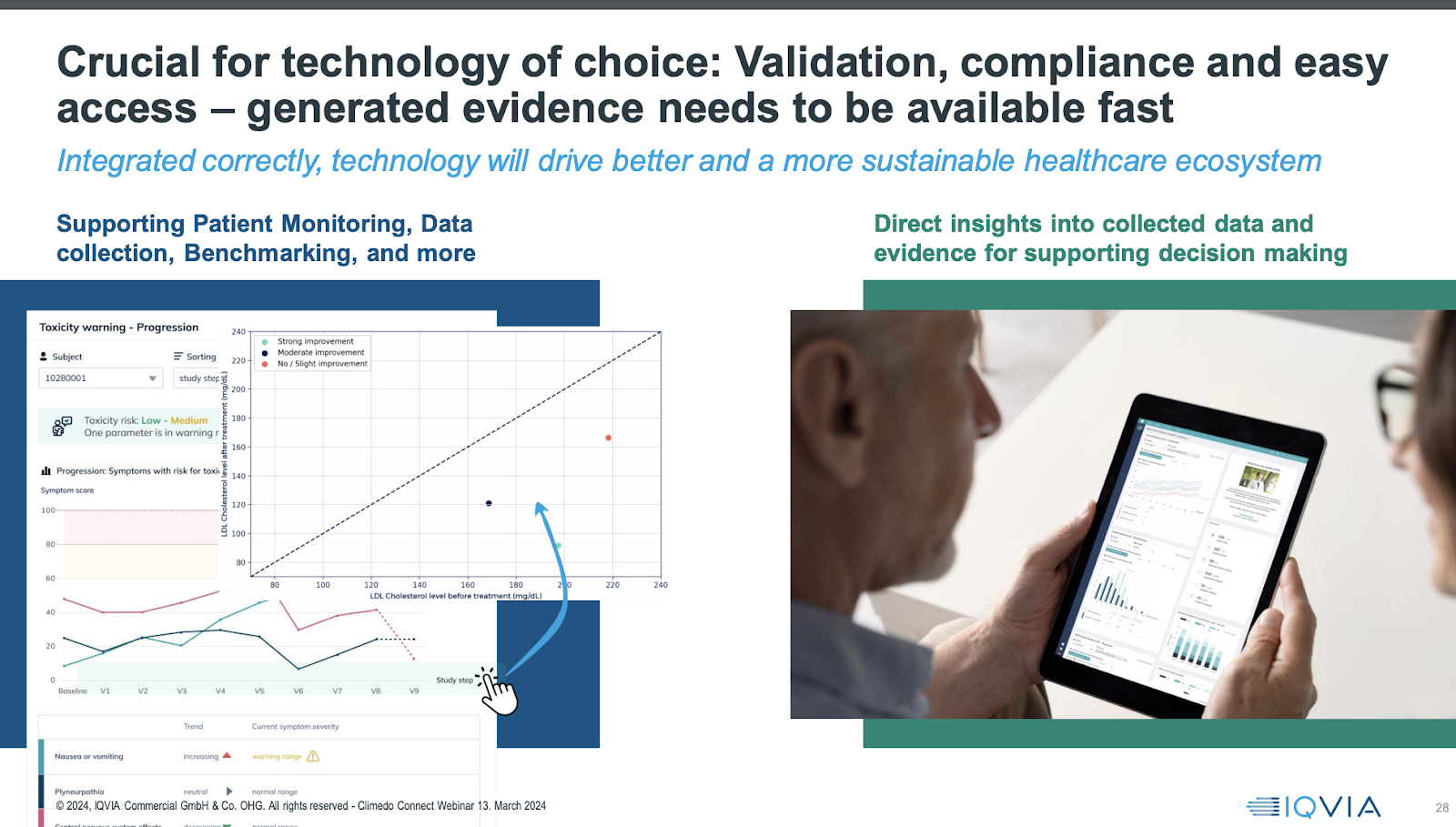
On the right, transparent communication with patients is facilitated through real-time access to their reported outcomes, as demonstrated in over 200 clinics in Germany. Patients become active participants in treatment decisions, fostering a collaborative approach between them and physicians.
This not only benefits patients and physicians but also extends to hospital quality departments and other stakeholders.
While these examples are specific, finding tailored solutions for your needs is essential. Despite the complexity of our industry, leveraging available options is now more accessible than ever. Adopting a pragmatic and transparent approach, even in requesting broad consent from patients, can yield significant benefits.
Reflecting on my experience with a study involving 10,000 hip/knee replacement patients, obtaining consent for data donation yielded a 93% approval rate. Transparent and well-informed data practices instill confidence and drive ROI across all phases.
In conclusion, data utilization is only effective when complemented by robust planning and interpretation methods. Addressing the myriad of questions surrounding this topic requires collaborative efforts. At IQVIA, we’re committed to continuing this conversation and addressing any further inquiries you may have in the remaining time.
Thank you for your attention today, I hope this presentation gave you some useful new insights!
Want to learn more about Climedo’s and IQVIA’s joint offering? Drop us a line.
* This blog post is based on a Climedo webinar from March 13, 2024 and was not released separately by IQVIA.

Catherine | Associate Director Marketing
Climedo
Passionate about creating innovative event and content marketing formats to make the benefits of digital health solutions more tangible. Enjoys fine art, photography, foreign languages and all things digital.
You may also like these articles



